Block the Ban
The New Zealand government has announced it is banning puberty blockers for transgender youth. As a 'Middle Aged White Guy' why do I care?


I'm going to 'outsource' much of this post to those who know far more than I:
What are puberty blockers, and gender affirming care?

What is the Ban?
This, quote from the PinkNews article linked below, summarises the ban:
The New Zealand government has announced it is banning puberty blockers for transgender youth as it awaits the results of a major clinical trial in the UK – which are not expected until 2031.
The announcement means that, from 19 December, any new prescriptions of hormone suppressing drugs – known as gonadotropin-releasing hormone analogues – for the treatment of gender dysphoria will be halted.
However, the drugs will remain available to trans youth with existing prescriptions, and those who require them for the treatment of early-onset puberty, endometriosis and prostate cancer, or where “clinical evidence clearly demonstrates their benefit”.

What is the Motivation?
It's political, purely political. Rational debate does not use this language:
Puberty blocker legislation is not based on politics.
It’s based on keeping our kids safe from woke ideological ferals who think it’s ok to expose vulnerable children to unsafe and unproven chemicals.
It’s based on letting kids be kids and stopping turning our society into a plaything for extremist lefty losers.
https://www.facebook.com/winstonpeters/posts/

Why do I care?
It's in the 'Doesn't impact me directly, but I feel for those it does, and fear where it might lead' space for me. Politicians overriding health professionals is a bad thing:

What can you do?
On Sunday I joined 'Block the Ban' to march in Auckland's CBD. It was a great event. A peaceful march bookended by speeches sharing personal, professional, and organisational impacts of the ban.





Block the Ban are planning future events and have links to resources here:

Contacts and information for Block The Ban
For a more general look at Trans Rights issues, consider Matt's short podcast series:

Learn...
Postscript: But what about 'The Cass Report'?
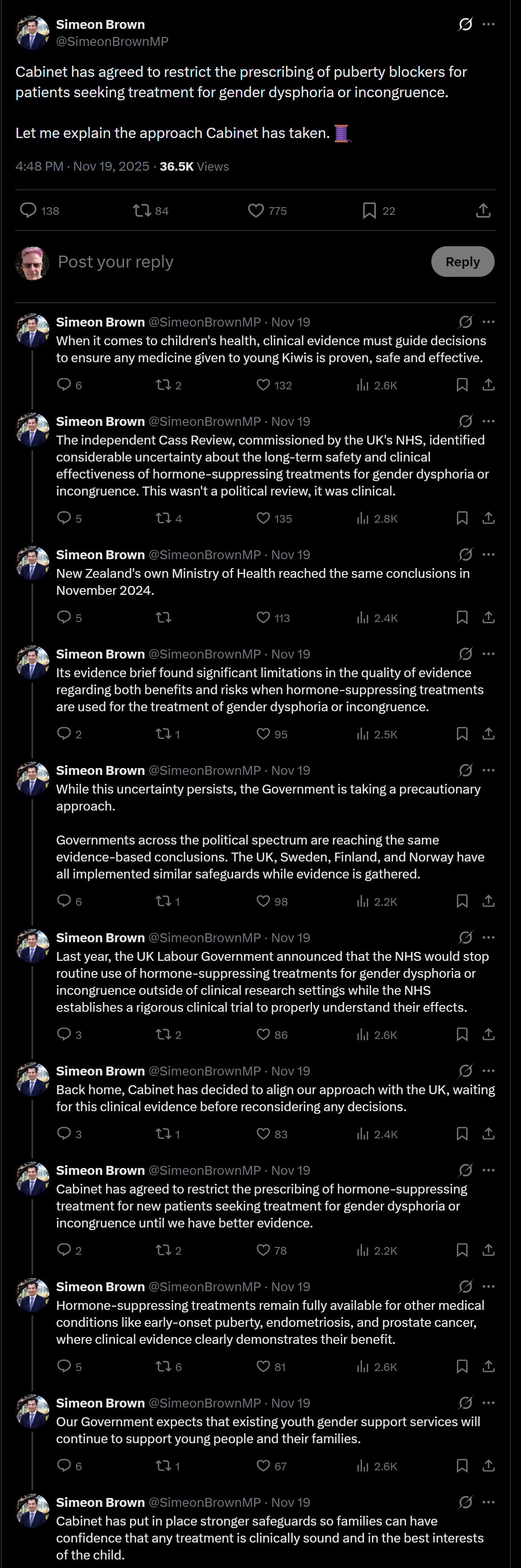
This is often cited, even by our Health Minister to justify this act:
On Wednesday (19 November) NZ’s health minister Simeon Brown wrote in a statement shared on X.com [see screen capture below] that the government is taking “a precautionary approach” and cited the UK’s controversial Cass Review as justification for the ban.
We are basing our policy on a deeply flawed U.K. study?
Critically appraising the cass report: methodological flaws and unsupported claims.
Noone, C., Southgate, A., Ashman, A. et al. | BMC Med Res Methodol 25, 128 (2025).
Conclusions
We have demonstrated that the Cass report’s application of EBM to GAC for children and young people is deeply flawed. Our critical analysis reveals significant methodological problems in the commissioned systematic reviews and primary research that undermine the validity of the Cass report’s recommendations. During our review of the report and supplementary primary research, we found insufficient statistical rigor, unreliable datasets, claims presented without evidence, and misrepresentation of quotes from primary research participants.
These flaws highlight a potential double standard present throughout the review and its subsequent recommendations, where evidence for gender-affirming care is held to a higher standard than the evidence used to support many of the report’s recommendations. Considering this, and the Cass report’s poor understanding of transgender identities and experiences, it is vital to question the integrity and validity of the Review’s recommendations and the appropriateness of basing health policy on them.
To uphold its commitment to evidence-based medicine, future gender-affirming care research must generate robust observational data, involve transgender communities, and prioritise patient-centred outcomes, ensuring validity, generalisability, and cultural relevance.